September 5, 2020, by Dr. Naveen Acharya, MD, FACC
Introduction:
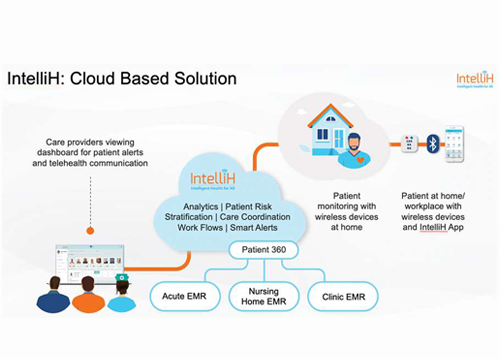
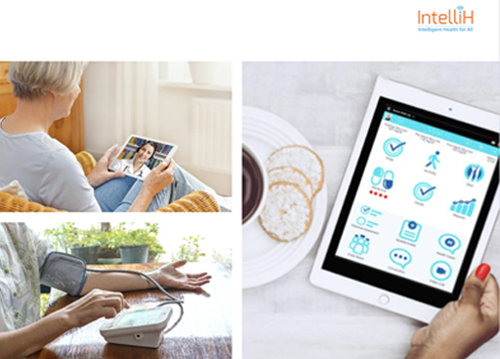
IntelliH is a comprehensive, workflow-based remote patient monitoring (RPM) system. It assimilates patient generated data from simple wireless sensors through a mobile App and using analytics built into a web-based care-coordinator dashboard, makes correlations with a variety of clinical and lifestyle factors. Telehealth is embedded within the solution to provide education and feedback to patients in the context of the data that has been captured through the monitoring platform.
RPM for heart failure:
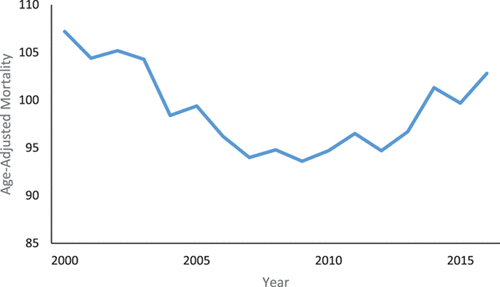
RPM, in smaller, nonrandomized trials, has been shown to reduce heart failure admissions and to lower all-cause mortality. However, these benefits have not been shown consistently in larger randomized trials.2-7 Two themes, however, have emerged: First, the benefits of RPM are best achieved when RPM platforms operate in the context of well-established clinical workflows with the immediate notice of alerts combined with the necessary mechanisms to provide an appropriate response 1,16. Second, RPM solutions are most successful when they are designed to better enable the needs of the users by appealing to a wide range of ages and digital acumen. This means not just facilitating a better user experience for patients but also for care coordinators with better integration to existing workflows already embedded within established electronic health record systems 8-16.
IntelliH for CHF:
The IntelliH care-coordinator dashboard has been designed to utilize the best workflows and practices used in most cardiology clinics:
- We understand that clinics employ multiple staff members, who aggregate in teams to provide the best care for patients. IntelliH facilitates better communication between care team members and allows the delegation of tasks as appropriate. Because the care team may also encompass family members IntelliH has constructed a dedicated app that enables family members to participate in the treatment plan. Cohorts of patients can also be assigned to care teams according to their weekly shift.
- Risk stratification tools are built into the system to enable care teams to appropriately assign resources to patients most at risk for disease decompensation.
- Alerts are displayed in real-time leveraging the cloud-based software architecture. Alert forwarding to other team members is also possible to involve the best available clinical resources. Dry weight can be programmed in order to create appropriate range-based alerts.
- HIPAA compliant communication mechanisms including secured chat and video conferencing allow immediate clinical responses to alerts. Embedded note taking tools allow better record-keeping.
- IntelliH is built on a multi-user architecture that allows multiple professionals to be on the system at the same time analyzing vitals data cohesively. Multi-party video conferencing facilitates multidisciplinary care. This is especially useful for CHF patients with uncontrolled glucose levels. These patients can be managed by multi-specialty teams of cardiologists, endocrinologists, and Diabetes educators.
- The care coordination web-based dashboard is available on tablets to keep clinical teams mobile, with push notifications arriving on the lock screen to enable rapid triage of alerts.
- IntelliH is integrated with the Epic EMR system; registration data including demographic information as well as medication lists can be directly imported from Epic into the IntelliH web-based dashboard, which has the ability to seamlessly transmit the relevant data to patients’ apps via their care plans.
IntellIH is able to interface with patients using the mobile app, which incorporates several innovative features, to enhance the patient’s user experience. These include:
- Utility of the smart phone dictation and tap features to minimize the need to type in data.
- Availability on larger tablet screens to improve the display visibility, particularly for elderly patients.
- Detailed voice instructions to guide vitals gathering from Bluetooth sensors.
- Rapid intake of medication compliance.
- Picture based dietary information capture.
- Comprehensive care plans
- Dynamic vitals gathering according to the chronic diseases being managed.
- Disease specific questionnaires to monitor relevant symptoms.
- Ad hoc video conferencing with care givers.
- Seamless connectivity with family members.
To summarize, IntelliH uses state-of-the-art Bluetooth connectivity tools to digitally gather vitals from patients in the least intrusive manner possible. Yet, simply collecting vitals from patients is only half the story of a remote patient monitoring system. It is the care-coordination aspect of the platform and ability to engage multiple members of the care team that drives successful adoption and scalability in a health system. Thus, consistent with clinical trials, the biggest strength of the system is the ability to easily fit into the operations and existing well-established workflows of a cardiology clinic.
The system was conceived with a multidisciplinary clinical team in mind where multiple clinical resources can be gathered, through the technology, around the patient to rapidly respond in real-time to out-of-bound vitals that may trigger alerts. The patient-proven user experience of the mobile app along with the workflow driven care coordinator web-based system, is the greatest asset of a cardiology clinic: The patient-caregiver relationship, which ultimately when strengthened is the best driver of improved clinical outcomes.
Dr. Naveen Acharya is a practicing cardiologist in Florida and the Chief Medical Officer of IntelliH.
References:
- AHA position paper 2019: Using Remote Patient Monitoring Technologies for Better Cardiovascular Disease Outcomes Guidance
- Saxon LA, Hayes DL, Gilliam FR, Heidenreich PA, Day J, Seth M, Meyer TE, Jones PW and Boehmer JP. Long-term outcome after ICD and CRT implantation and influence of remote device follow-up: the ALTITUDE survival study. Circulation. 2010;122:2359-67.
- Varma N, Piccini JP, Snell J, Fischer A, Dalal N and Mittal S. The Relationship Between Level of Adherence to Automatic Wireless Remote Monitoring and Survival in Pacemaker and Defibrillator Patients. J Am Coll Cardiol. 2015;65:2601-2610.
- De Simone A, Leoni L, Luzi M, Amellone C, Stabile G, La Rocca V, Capucci A, D’Onofrio A, Ammendola E, Accardi F, Valsecchi S and Buja G. Remote monitoring improves outcome after ICD implantation: the clinical efficacy in the management of heart failure (EFFECT) study. Europace. 2015;17:1267-75.
- Portugal G, Cunha P, Valente B, Feliciano J, Lousinha A, Alves S, Braz M, Pimenta R, Delgado AS, Oliveira M and Ferreira RC. Influence of remote monitoring on long-term cardiovascular outcomes after cardioverterdefibrillator implantation. Int J Cardiol. 2016;222:764-768.
- Kurek A, Tajstra M, Gadula-Gacek E, Buchta P, Skrzypek M, Pyka L, Wasiak M, Swietlinska M, Hawranek M, Polonski L, Gasior M and Kosiuk J. Impact of Remote Monitoring on Long- Term Prognosis in Heart Failure Patients in a Real-World Cohort: Results From All-Comers COMMIT-HF Trial. J Cardiovasc Electrophysiol. 2017;28:425-431.
- Piccini JP, Mittal S, Snell J, Prillinger JB, Dalal N and Varma N. Impact of remote monitoring on clinical events and associated health care utilization: A nationwide assessment. Heart Rhythm. 2016;13:2279-2286.
- Goldberg L, Lide B, Lowry S, Massett HA, O’Connell T, Preece J, Quesenbery W and Shneiderman B. Usability and accessibility in consumer health informatics current trends and future challenges. Am J Prev Med. 2011;40:S187-97.
- Jaspers MW. A comparison of usability methods for testing interactive health technologies: methodological aspects and empirical evidence. Int J Med Inform. 2009;78:340-53.
- Scherr D, Kastner P, Kollmann A, Hallas A, Auer J, Krappinger H, Schuchlenz H, Stark G, Grander W, Jakl G, Schreier G, Fruhwald FM and Investigators M. Effect of home-based telemonitoring using mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation: randomized controlled trial. J Med Internet Res. 2009;11:e34.
- Goldberg LR, Piette JD, Walsh MN, Frank TA, Jaski BE, Smith AL, Rodriguez R, Mancini DM, Hopton LA, Orav EJ, Loh E and Investigators W. Randomized trial of a daily electronic home monitoring system in patients with advanced heart failure: the Weight Monitoring in Heart Failure (WHARF) trial. Am Heart J. 2003;146:705-12.
- Cleland JG, Louis AA, Rigby AS, Janssens U, Balk AH and Investigators T-H. Noninvasive home telemonitoring for patients with heart failure at high risk of recurrent admission and death: the Trans-European Network-HomeCare Management System (TEN-HMS) study. J Am Coll Cardiol. 2005;45:1654-64.
- Koppel R, Metlay JP, Cohen A, Abaluck B, Localio AR, Kimmel SE and Strom BL. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293:1197-203.
- Ash JS, Berg M and Coiera E. Some unintended consequences of information technology in health care: the nature of patient care information system-related errors. Journal of the American Medical Informatics Association. 2004;11:104-112.
- Rahimi K, Velardo C, Triantafyllidis A, Conrad N, Shah SA, Chantler T, Mohseni H, Stoppani E, Moore F, Paton C, Emdin CA, Ernst J, Tarassenko L, Investigators S-H, Rahimi K, Velardo
- DesaiAS, StevensonLW. Connecting the circle from home to heart-failure disease management. N Engl J Med 2010; 363: 2364–2367.
Share This blog