Summarized from: Heart Rate Variability Standards of Measurement, Physiological Interpretation, and Clinical Use Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology Originally published 1 Mar 1996
Source: Adv Physiol Educ 43: 270–276, 2019; doi:10.1152/advan.00019.2019
SDNN

SDANN
Calculated from segments of the total monitoring period, SDANN, the standard deviation of the average NN intervals calculated over short periods, usually 5 minutes, which is an estimate of the changes in heart rate due to cycles longer than 5 minutes, and the SDNN index, the mean of the 5-minute standard deviations of NN intervals calculated over 24 hours, which measures the variability due to cycles shorter than 5 minutes.
RMSSD

Derived from interval differences RMSSD is the square root of the mean squared differences of successive NN intervals. Used by Fitbit devices.
NN50 and pNN50
NN50, the number of interval differences of successive NN intervals greater than 50 ms, and pNN50, the proportion derived by dividing NN50 by the total number of NN intervals. All of these measurements of short-term variation estimate high-frequency variations in heart rate and thus are highly correlated.
The HRV triangular index
This measurement is the integral of the density distribution (that is, the number of all NN intervals) divided by the maximum of the density distribution. Using a measurement of NN intervals on a discrete scale, the measure is approximated by the value (total number of NN intervals)/(number of NN intervals in the modal bin), which is dependent on the length of the bin, that is, on the precision of the discrete scale of measurement.
The triangular interpolation of NN interval histogram (TINN)
This is the baseline width of the distribution measured as a base of a triangle approximating the NN interval distribution (the minimum square difference is used to find such a triangle).
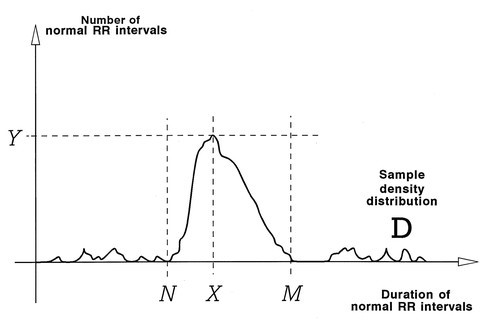
To perform geometric measures on the NN interval histogram, the sample density distribution D is constructed, which assigns the number of equally long NN intervals to each value of their lengths. The most frequent NN interval length X is established, that is, Y=D(X) is the maximum of the sample density distribution D. The HRV triangular index is the value obtained by dividing the area integral of D by the maximum Y.
For the computation of the TINN measure, the values N and M are established on the time axis and a multilinear function q constructed such that q(t)=0 for t≤N and t≥M and q(X)=Y, and such that the integral ∫0+∞ (D(t)−q(t))2 dt is the minimum among all selections of all values N and M. The TINN measure is expressed in milliseconds and given by the formula TINN=M−N. Also see Table 1.
|
Variable |
Units |
Description |
|---|---|---|
|
Statistical Measures |
||
|
SDNN |
ms |
Standard deviation of all NN intervals |
|
SDANN |
ms |
Standard deviation of the averages of NN intervals in all 5-minute segments of the entire recording |
|
RMSSD |
ms |
The square root of the mean of the sum of the squares of differences between adjacent NN intervals |
|
SDNN index |
ms |
Mean of the standard deviations of all NN intervals for all 5-minute segments of the entire recording |
|
SDSD |
ms |
Standard deviation of differences between adjacent NN intervals |
|
NN50 count |
Number of pairs of adjacent NN intervals differing by more than 50 ms in the entire recording; three variants are possible counting all such NN intervals pairs or only pairs in which the first or the second interval is longer |
|
|
pNN50 |
% |
NN50 count divided by the total number of all NN intervals |
|
Geometric Measures |
||
|
HRV triangular index |
Total number of all NN intervals divided by the height of the histogram of all NN intervals measured on a discrete scale with bins of 7.8125 ms (1/128 seconds) (details in Fig 2) |
|
|
TINN |
ms |
Baseline width of the minimum square difference triangular interpolation of the highest peak of the histogram of all NN intervals (details in Fig 2) |
|
Differential index |
ms |
Difference between the widths of the histogram of differences between adjacent NN intervals measured at selected heights (eg, at the levels of 1000 and 10 000 samples)20 |
|
Logarithmic index |
ms |
Coefficient φ of the negative exponential curve k · e−φt, which is the best approximation of the histogram of absolute differences between adjacent NN intervals21 |
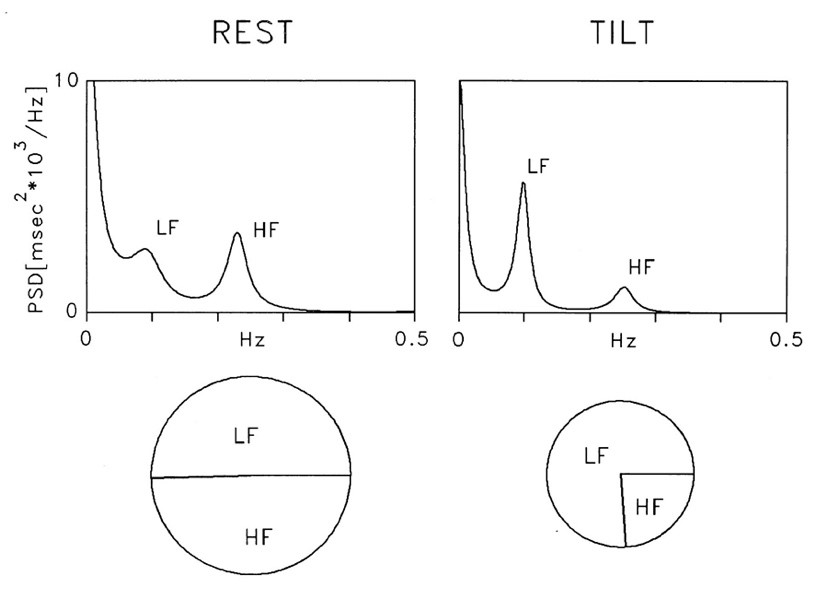
Spectral analysis (autoregressive model, order 12) of RR interval variability in a healthy subject at rest and during 90° head-up tilt. At rest, two major components of similar power are detectable at low and high frequencies. During tilt, the LF component becomes dominant, but as total variance is reduced, the absolute power of LF appears unchanged compared with rest. Normalization procedure leads to predominant LF and smaller HF components, which express the alteration of spectral components due to tilt
|
Variable |
Units |
Description |
Frequency Range |
|---|---|---|---|
|
Analysis of Short-term Recordings (5 min) |
|||
|
5-min total power |
ms2 |
The variance of NN intervals over the temporal segment |
≈≤0.4 Hz |
|
VLF |
ms2 |
Power in VLF range |
≤0.04 Hz |
|
LF |
ms2 |
Power in LF range |
0.04-0.15 Hz |
|
LF norm |
nu |
LF power in normalized units LF/(total power−VLF)×100 |
|
|
HF |
ms2 |
Power in HF range |
0.15-0.4 Hz |
|
HF norm |
nu |
HF power in normalized units HF/(total power−VLF)×100 |
|
|
LF/HF |
Ratio LF [ms2]/HF[ms2] |
||
|
Analysis of Entire 24 Hours |
|||
|
Total power |
ms2 |
Variance of all NN intervals |
≈≤0.4 Hz |
|
ULF |
ms2 |
Power in the ULF range |
≤0.003 Hz |
|
VLF |
ms2 |
Power in the VLF range |
0.003-0.04 Hz |
|
LF |
ms2 |
Power in the LF range |
0.04-0.15 Hz |
|
HF |
ms2 |
Power in the HF range |
0.15-0.4 Hz |
|
α |
Slope of the linear interpolation of the spectrum in a log-log scale |
≈≤0.04 Hz |
Normal Values of Standard Measures of HRV
|
Variable |
Units |
Normal Values (mean±SD) |
|---|---|---|
|
Time Domain Analysis of Nominal 24 hours181 |
||
|
SDNN |
ms |
141±39 |
|
SDANN |
ms |
127±35 |
|
RMSSD |
ms |
27±12 |
|
HRV triangular index |
37±15 |
|
|
Spectral Analysis of Stationary Supine 5-min Recording |
||
|
Total power |
ms2 |
3466 ±1018 |
|
LF |
ms2 |
1170±416 |
|
HF |
ms2 |
975±203 |
|
LF |
nu |
54±4 |
|
HF |
nu |
29±3 |
|
LF/HF ratio |
1.5-2.0 |
Summary of Selected Studies Investigating Clinical Value of HRV in Cardiological Diseases Other Than Myocardial Infarction
|
Disease State |
Author of Study |
Population (No. of Patients) |
Investigation Parameter |
Clinical Finding |
Potential Value |
|---|---|---|---|---|---|
|
Hypertension |
Guzzetti et al, 1991149 |
49 hypertensive 30 normals |
Spectral AR |
⇑LF found in hypertensives compared with normals with blunting of circadian patterns |
Hypertension is characterized by a depressed circadian rhythmicity of LF |
|
Langewitz et al, 1994 150 |
41 borderline hypertensive 34 hypertensive 54 normals |
Spectral FFT |
Reduced parasympathetic in hypertensive patients |
Support the use of nonpathological therapy of hypertension that ⇑ vagal tone (eg, exercise) |
|
|
CHF |
Saul et al, 1988151 |
25 chronic CHF NYHA III,IV 21 normals |
Spectral Blackman-Tukey 15-min acquisition |
⇓Spectral power all frequencies, especially >0.04 Hz in CHF patients |
In CHF, there is ⇓ vagal but relatively preserved sympathetic modulation of HR |
|
Casolo et al, 1989102 |
20 CHF NYHA II,III,IV 20 normals |
Time domain RR interval histogram with 24-h Holter |
Low HRV |
Reduced vagal activity in CHF patients |
|
|
Binkley et al, 1991152 |
10 dilated cardiomyopathy (EF 14% to 40%) 10 normals |
Spectral FFT 4-min supine acquisition |
⇓HF power (>0.1 Hz) in CHF ⇑LF/HF |
Withdrawal of parasympathetic tone observed in CHF. CHF has imbalance of autonomic tone with ⇓ parasympathetic and a predominance of sympathetic tone |
|
|
Kienzle et al, 1992104 |
23 CHF NYHA II,III,IV |
Spectral FFT Time domain 24-48-h Holter |
Alterations of HRV not tightly linked to severity of CHF ⇓HRV was related to sympathetic excitation |
||
|
Townend et al, 1992153 |
12 CHF NYHA III,IV |
Time domain 24-h Holter |
HRV⇑ during ACE inhibitor treatment |
||
|
Binkley et al, 1993154 |
13 CHF NYHA II,III |
Spectral FFT 4-min supine acquisition |
12 weeks of ACE inhibitor treatment ⇑HF HRV |
Significant augmentation of parasympathetic tone was associated with ACE inhibitor therapy |
|
|
Woo et al, 1994155 |
21 CHF NYHA III |
Poincaré plots Time domain 24-h Holter |
Complex plots are associated with ⇑norepinephrine levels and greater sympathetic activation |
Poincaré plots may assist analysis of sympathetic influences |
|
|
Heart transplantation |
Alexopoulos et al, 1988156 |
19 transplant 10 normals |
Time domain 24-h Holter |
Reduced HRV in denervated donor hearts; recipient innervated hearts had more HRV |
|
|
Sands et al, 1989100 |
17 transplant 6 normals |
Spectral FFT 15-min supine acquisition |
HRV from 0.02 to 1.0 Hz; 90% reduced |
Patients with rejection documented biopsy show significantly more variability |
|
|
Chronic mitral regurgitation |
Stein et al, 1993157 |
38 chronic mitral regurgitation |
Spectral FFT Time domain 24-h Holter |
HR and measures of ULF by SDANN correlated with ventricular performance and predicted clinical events |
May be prognostic indicator of atrial fibrillation, mortality, and progression to valve surgery |
|
Mitral valve prolapse |
Marangoni et al, 1993158 |
39 female mitral valve prolapse 24 female controls |
Spectral AR 10-min supine acquisition |
MVP patients had ⇓HF |
MVP patients had low vagal tone |
|
Cardiomyopathies |
Counihan et al, 1993159 |
104 HCM |
Spectral FFT Time domain 24-h Holter |
Global and specific vagal tone measurements of HRV were ⇓ in symptomatic patients |
HRV does not add to the predictive accuracy of known risk factors in HCM |
|
SD or CA |
Dougherty et al, 1992160 |
16 CA survivors 5 CA nonsurvivors 5 normals |
Spectral AR Time domain 24-h Holter |
HRV as measured by LF power and SDNN were significantly related to 1-y mortality |
HRV is clinically useful to risk stratify CA survivors for 1-y mortality |
|
Huikuri et al, 1992161 |
22 CA survivors 22 control |
Spectral AR Time domain 24-h Holter |
⇓HF power in CA survivors; LF power did not discriminate CA survivors Circadian pattern of HRV found in all patients |
||
|
Algra et al, 1993110 |
193 SD cases 230 symptomatic patients |
Time domain 24-h Holter |
⇓Short-term variation (0.05-0.50 Hz) independently increased the risk of SD by a factor of 2.6 ⇓Long-term variation (0.02-0.05 Hz) increased the risk of SD by a factor of 2 |
HRV may be used to estimate the risk of SD |
ACE indicates angiotensin-converting enzyme; AR, autoregressive; CA, cardiac arrest; CAD, coronary artery disease; CHF, congestive heart failure; EF, ejection fraction; FFT, fast Fourier transform; HCM, hypertrophic cardiomyopathy; HF, high frequency; HRV heart rate variability; LF, low frequency; MVP, mitral valve prolapse; NYHA, New York Heart Association classification; SD, sudden death; SVT, supraventricular tachycardia; VF, ventricular fibrillation; and VT, ventricular tachycardia.
Continued
|
Disease State |
Author of Study |
Population (No. of Patients) |
Investigation Parameter |
Clinical Finding |
Potential Value |
|---|---|---|---|---|---|
|
Myers et al, 1986162 |
6 normals 12 patients with structural heart disease (6 with and 6 without SD) |
Time and frequency domain 24-h Holter |
Both time and frequency domain indices separated normals from SD patients ⇓HF power (0.35-0.5 Hz) was the best separator between heart disease patients with and without SD |
HF power may be a useful predictor of SD |
|
|
Martin et al, 1986163 |
20 normals 5 patients experiencing SD during Holter monitoring |
Time domain 24-h Holter |
SDNN index significantly lower in SD patients |
Time domain indices may identify increased risk of SD |
|
|
Ventricular arrhythmias |
Vybiral et al, 1993164 |
24 VF |
Time domain 24-h Holter |
HRV indices do not change consistently before VF |
|
|
Huikuri et al, 1993165 |
18 VT or CA |
Spectral AR 24-h Holter |
All power spectra of HRV were significantly ⇓ before the onset of sustained VT than before nonsustained VT |
A temporal relation exists between the decrease of HRV and the onset of sustained VT |
|
|
Hohnloser et al, 1994166 |
14 post-MI with VF or sustained 14 post-MI (matched) |
Spectral FFT Time domain 24-h Holter |
HRV of post MI-CA survivors do not differ from other post MI patients; they differ strikingly in terms of baroreflex sensitivity |
Baroreflex sensitivity, not HRV, distinguished post-MI patients with and without VF and VT |
|
|
Supraventricular arrhythmias |
Kocovic et al, 1993167 |
64 SVT |
Spectral FFT Time domain 5-min supine acquisition 24-h Holter |
⇑HR,⇓HRV, and ⇓parasympathetic components after radiofrequency ablation |
Parasympathetic ganglia and fibers may be more dense in the mid and anterior low septum |
Share This blog